Overview
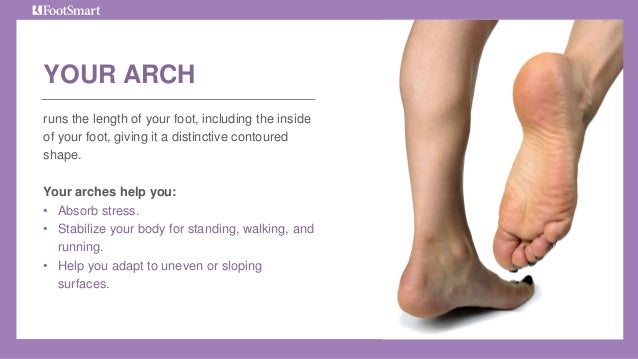
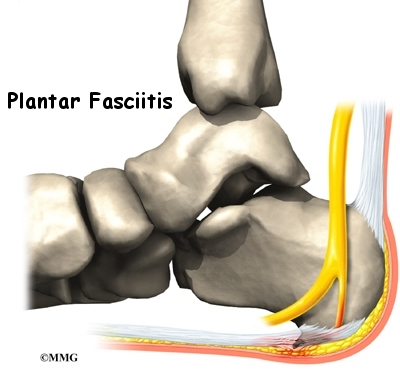
The adult acquired flatfoot (AAF) is a progressive, symptomatic (painful) deformity resulting from gradual stretch (attenuation) of the tibialis posterior tendon as well as the ligaments that support the arch of the foot. Although the posterior tibialis tendon plays a significant role, this pathology has recently been recognized as involving failure of other interosseous ligaments, such as the spring ligament. Due to the complexity of this pathology, posterior tibial tendon dysfunction (PTTD) is now referred to as adult acquired flatfoot. Severe flatfoot associated with AAF can lead to other problems, such as plantar fascial tension, tendon pain, rearfoot subluxation, and ankle osteoarthritis.
Causes
As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch.
Symptoms
Initially, flatfoot deformity may not present with any symptoms. However, overtime as the tendon continues to function in an abnormal position, people with fallen arches will begin to have throbbing or sharp pain along the inside of the arch. Once the tendon and soft tissue around it elongates, there is no strengthening exercises or mechanism to shorten the tendon back to a normal position. Flatfoot can also occur in one or both feet. If the arch starts to slowly collapse in one foot and not the other, posterior tibial dysfunction (PTTD) is the most likely cause. People with flatfoot may only have pain with certain activities such as running or exercise in the early phase of PTTD. Pain may start from the arch and continue towards the inside part of the foot and ankle where the tendon courses from the leg. Redness, swelling and increased warmth may also occur. Later signs of PTTD include pain on the outside of the foot from the arch collapsing and impinging other joints. Arthritic symptoms such as painful, swollen joints in the foot and ankle may occur later as well due to the increased stress on the joints from working in an abnormal position for a long period of time.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
Initial treatment for most patients consists of rest and anti-inflammatory medications. This will help reduce the swelling and pain associated with the condition. The long term treatment for the problem usually involves custom made orthotics and supportive shoe gear to prevent further breakdown of the foot. ESWT(extracorporeal shock wave therapy) is a novel treatment which uses sound wave technology to stimulate blood flow to the tendon to accelerate the healing process. This can help lead to a more rapid return to normal activities for most patients. If treatment is initiated early in the process, most patients can experience a return to normal activities without the need for surgery.
Surgical Treatment
The indications for surgery are persistent pain and/or significant deformity. Sometimes the foot just feels weak and the assessment of deformity is best done by a foot and ankle specialist. If surgery is appropriate, a combination of soft tissue and bony procedures may be considered to correct alignment and support the medial arch, taking strain off failing ligaments. Depending upon the tissues involved and extent of deformity, the foot and ankle specialist will determine the necessary combination of procedures. Surgical procedures may include a medial slide calcaneal osteotomy to correct position of the heel, a lateral column lengthening to correct position in the midfoot and a medial cuneiform osteotomy or first metatarsal-tarsal fusion to correct elevation of the medial forefoot. The posterior tibial tendon may be reconstructed with a tendon transfer. In severe cases (stage III), the reconstruction may include fusion of the hind foot,, resulting in stiffness of the hind foot but the desired pain relief. In the most severe stage (stage IV), the deltoid ligament on the inside of the ankle fails, resulting in the deformity in the ankle. This deformity over time can result in arthritis in the ankle.
The adult acquired flatfoot (AAF) is a progressive, symptomatic (painful) deformity resulting from gradual stretch (attenuation) of the tibialis posterior tendon as well as the ligaments that support the arch of the foot. Although the posterior tibialis tendon plays a significant role, this pathology has recently been recognized as involving failure of other interosseous ligaments, such as the spring ligament. Due to the complexity of this pathology, posterior tibial tendon dysfunction (PTTD) is now referred to as adult acquired flatfoot. Severe flatfoot associated with AAF can lead to other problems, such as plantar fascial tension, tendon pain, rearfoot subluxation, and ankle osteoarthritis.
Causes
As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch.
Symptoms
Initially, flatfoot deformity may not present with any symptoms. However, overtime as the tendon continues to function in an abnormal position, people with fallen arches will begin to have throbbing or sharp pain along the inside of the arch. Once the tendon and soft tissue around it elongates, there is no strengthening exercises or mechanism to shorten the tendon back to a normal position. Flatfoot can also occur in one or both feet. If the arch starts to slowly collapse in one foot and not the other, posterior tibial dysfunction (PTTD) is the most likely cause. People with flatfoot may only have pain with certain activities such as running or exercise in the early phase of PTTD. Pain may start from the arch and continue towards the inside part of the foot and ankle where the tendon courses from the leg. Redness, swelling and increased warmth may also occur. Later signs of PTTD include pain on the outside of the foot from the arch collapsing and impinging other joints. Arthritic symptoms such as painful, swollen joints in the foot and ankle may occur later as well due to the increased stress on the joints from working in an abnormal position for a long period of time.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
Initial treatment for most patients consists of rest and anti-inflammatory medications. This will help reduce the swelling and pain associated with the condition. The long term treatment for the problem usually involves custom made orthotics and supportive shoe gear to prevent further breakdown of the foot. ESWT(extracorporeal shock wave therapy) is a novel treatment which uses sound wave technology to stimulate blood flow to the tendon to accelerate the healing process. This can help lead to a more rapid return to normal activities for most patients. If treatment is initiated early in the process, most patients can experience a return to normal activities without the need for surgery.
Surgical Treatment
The indications for surgery are persistent pain and/or significant deformity. Sometimes the foot just feels weak and the assessment of deformity is best done by a foot and ankle specialist. If surgery is appropriate, a combination of soft tissue and bony procedures may be considered to correct alignment and support the medial arch, taking strain off failing ligaments. Depending upon the tissues involved and extent of deformity, the foot and ankle specialist will determine the necessary combination of procedures. Surgical procedures may include a medial slide calcaneal osteotomy to correct position of the heel, a lateral column lengthening to correct position in the midfoot and a medial cuneiform osteotomy or first metatarsal-tarsal fusion to correct elevation of the medial forefoot. The posterior tibial tendon may be reconstructed with a tendon transfer. In severe cases (stage III), the reconstruction may include fusion of the hind foot,, resulting in stiffness of the hind foot but the desired pain relief. In the most severe stage (stage IV), the deltoid ligament on the inside of the ankle fails, resulting in the deformity in the ankle. This deformity over time can result in arthritis in the ankle.
 The Achilles is a large tendon that connects two major calf muscles to the back of the heel bone. If this tendon is overworked and tightens, the collagen fibres of the tendon may break, causing inflammation and pain. This can result in scar tissue formation, a type of tissue that does not have the flexibility of tendon tissue. Four types of Achilles injuries exist, 1) Paratendonitis - involves a crackly or crepitus feeling in the tissues surrounding the Achilles tendon. 2) Proliferative Tendinitis - the Achilles tendon thickens as a result of high tension placed on it. 3) Degenerative Tendinitis - a chronic condition where the Achilles tendon is permanently damaged and does not regain its structure. 4) Enthesis - an inflammation at the point where the Achilles tendon inserts into the heel bone.
The Achilles is a large tendon that connects two major calf muscles to the back of the heel bone. If this tendon is overworked and tightens, the collagen fibres of the tendon may break, causing inflammation and pain. This can result in scar tissue formation, a type of tissue that does not have the flexibility of tendon tissue. Four types of Achilles injuries exist, 1) Paratendonitis - involves a crackly or crepitus feeling in the tissues surrounding the Achilles tendon. 2) Proliferative Tendinitis - the Achilles tendon thickens as a result of high tension placed on it. 3) Degenerative Tendinitis - a chronic condition where the Achilles tendon is permanently damaged and does not regain its structure. 4) Enthesis - an inflammation at the point where the Achilles tendon inserts into the heel bone.
 RSS Feed
RSS Feed
